
Breathing Under Pressure:
How Hyperbaric Oxygen Saves Lives in Carbon Monoxide Poisoning
When invisible fumes bind to the blood’s oxygen carriers, a century-old pressurised chamber treatment remains the most powerful tool medicine has to break that grip and prevent lasting brain damage.

Fig. 1 — Carbon monoxide (CO) binds to hemoglobin with approximately 240 times greater affinity than oxygen, forming carboxyhemoglobin (COHb) and rendering red blood cells unable to deliver oxygen to tissues.
Carbon monoxide poisoning is deceptive in its silence. The gas is invisible, odourless, and tasteless — yet it kills more people through accidental poisoning than any other single toxin in industrialised countries. Each year in the United States alone, roughly 50,000 emergency department visits are attributed to unintentional CO exposure, with more than 400 fatalities. Understanding why hyperbaric oxygen therapy (HBOT) is so effective requires following the molecular catastrophe that CO sets in motion inside the body.
When inhaled, carbon monoxide crosses from the lungs into the bloodstream within seconds. There, it encounters hemoglobin — the iron-containing protein in red blood cells whose entire purpose is to capture oxygen in the lungs and release it into tissues throughout the body. CO binds to the same iron site as oxygen, but with a ferocious affinity: roughly 240 times stronger. The resulting compound, carboxyhemoglobin (COHb), is a biological dead-end. The hemoglobin molecule, now locked in CO’s grip, cannot pick up oxygen — and it cannot easily let go of the CO either.
The Silent Cascade of Cellular Injury
The damage from CO goes far deeper than simply stealing haemoglobin’s carrying capacity. CO also enters cells directly, where it binds to cytochrome c oxidase — the final enzyme in the mitochondrial electron transport chain and the molecular engine that converts oxygen into cellular energy (ATP). When this enzyme is inhibited, cells cannot generate energy even if oxygen somehow reaches them. The heart and brain, being the organs most dependent on continuous oxygen delivery and ATP production, suffer first and most severely.
A particularly insidious consequence of CO poisoning is delayed neurological sequelae (DNS) — a syndrome in which patients who initially seem to recover fully develop new cognitive, psychiatric, and movement disorders days to weeks after exposure. Studies suggest DNS occurs in 10–30% of symptomatic CO poisoning cases, and it is thought to be driven by a post-exposure cascade of lipid peroxidation, mitochondrial dysfunction, and inflammatory injury in the white matter of the brain. HBOT is the only treatment shown to meaningfully reduce the risk of DNS.

The Physics of the Cure: Why Pressure Changes Everything
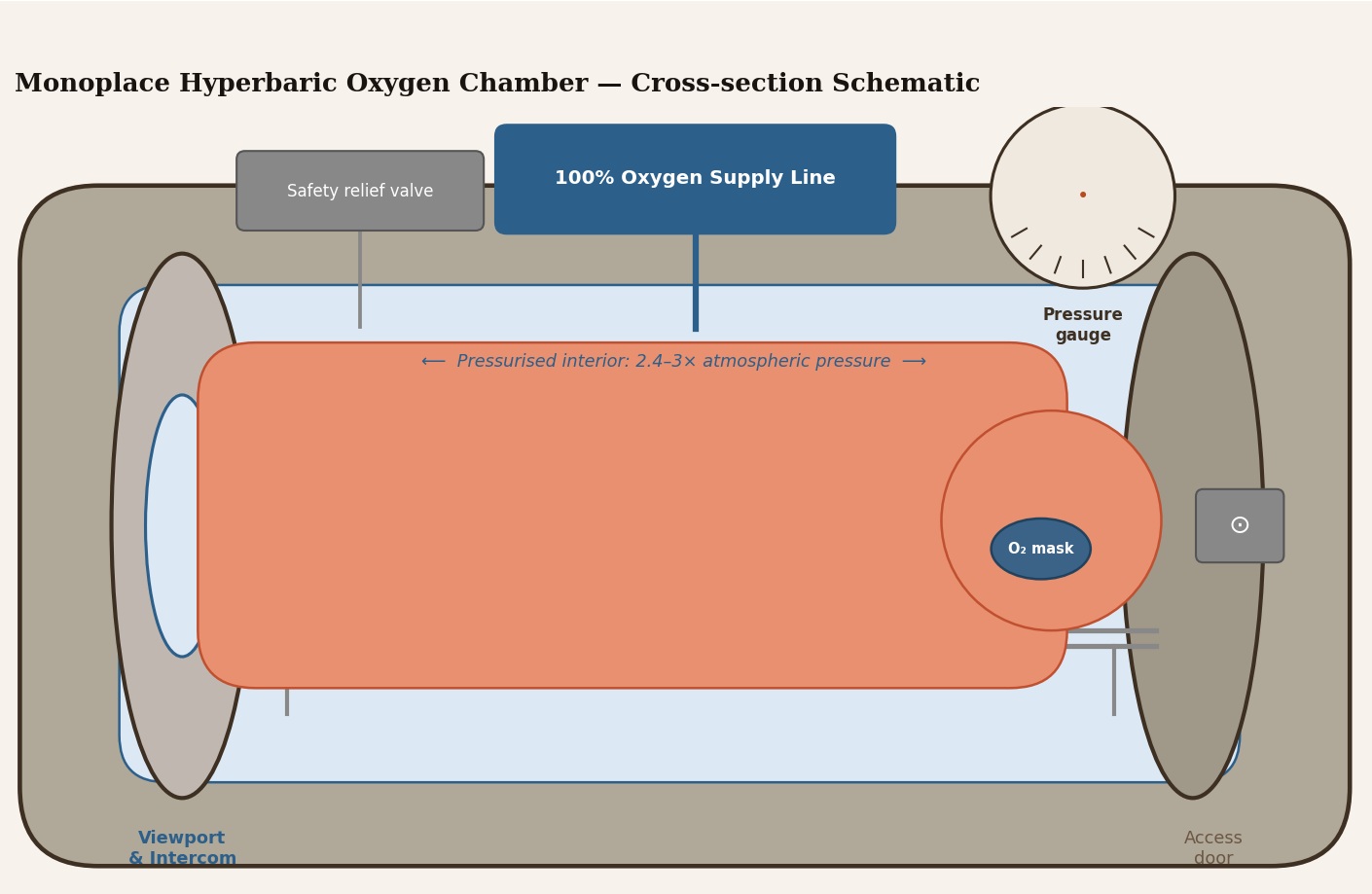
The hyperbaric oxygen chamber is, at its core, a physics problem made biological. By raising the ambient pressure to 2.4–3 times atmospheric (2.4–3 ATA), and simultaneously having the patient breathe 100% oxygen, clinicians exploit Henry’s Law: the amount of a gas dissolved in a liquid is proportional to the partial pressure of that gas above the liquid.
At 3 ATA breathing pure oxygen, the partial pressure of oxygen in the alveoli rises to approximately 2,000 mmHg — compared to around 100 mmHg at sea level on room air. This flood of dissolved oxygen plasma accomplishes two critical things simultaneously. First, it provides massive competition for the hemoglobin binding site, overwhelming CO’s affinity advantage and dramatically accelerating CO displacement. Second — and this is crucial — oxygen dissolves directly into blood plasma in sufficient quantities to sustain life even in the complete absence of functional hemoglobin. Tissues receive the oxygen they need while the hemoglobin is being freed from CO’s grip.
“At hyperbaric pressures, plasma-dissolved oxygen alone can sustain tissue viability — buying critical time while the blood is being rescued.”

Clinical Evidence and Indications for HBOT
The evidence base for HBOT in CO poisoning is robust enough that it is incorporated into guidelines from the Undersea and Hyperbaric Medical Society (UHMS), and clinical practice guidelines from multiple emergency medicine bodies worldwide. The landmark Weaver et al. trial (2002) demonstrated that three sessions of HBOT at 2.4 ATA, compared to normobaric oxygen, reduced cognitive sequelae at 6 weeks from 46% to 25% — essentially halving the rate of delayed neurological injury.
Accepted Indications for HBOT in CO Poisoning
- Loss of consciousness — any syncope or coma attributable to CO exposure, regardless of current COHb level
- Neurological signs — confusion, ataxia, seizure, focal deficits, or persistent headache not resolving on normobaric oxygen
- Cardiac involvement — ischaemic ECG changes, troponin elevation, or haemodynamic instability
- Pregnancy — foetal haemoglobin binds CO even more avidly; HBOT is indicated at lower thresholds
- COHb ≥ 25% — or ≥ 15–20% in children, the elderly, or those with cardiovascular disease
- End-organ dysfunction — metabolic acidosis (lactate elevation), elevated troponin, or persistent symptoms after high-flow O₂
Clinical note: COHb levels on arrival in the ED frequently underestimate the true peak exposure — time elapsed since removal from the CO source, pre-hospital oxygen administration, and the variable rate of CO elimination all confound the laboratory value. Clinical presentation must always take precedence over a single COHb reading.

Beyond Hemoglobin: The Neuroprotective Mechanisms
One of the most important insights of the past two decades is that CO poisoning is not merely an oxygen-deprivation injury. The gas is an active toxin that triggers a cascade of secondary injury processes that continue — and may even accelerate — after the CO itself has been cleared.
HBOT interrupts several of these cascades simultaneously. Research led by Stephen Thom at the University of Pennsylvania showed that CO activates a specific pathway in which xanthine oxidase generates superoxide radicals, which in turn cause polymorphonuclear leukocytes (neutrophils) to adhere to cerebral vascular endothelium. This adherence leads to release of proteases and reactive oxygen species, producing a pattern of brain injury resembling cerebral ischaemia-reperfusion injury. High-pressure oxygen disrupts this by preserving nitric oxide bioavailability and preventing the initial oxidase activation.
Protective mechanism: At 2.4–3 ATA, dissolved oxygen competitively antagonises CO’s binding to the active site of cytochrome c oxidase within mitochondria — directly restoring the cellular energy machinery even before all COHb has cleared from blood.
A second mechanism involves CO’s promotion of lipid peroxidation — oxidative damage to cell membranes — particularly in myelin sheaths of nerve fibres. Once initiated, this peroxidation cascade can propagate independently of CO, continuing long after the original exposure and producing the white-matter lesions seen on MRI in patients with DNS. HBOT appears to both suppress the initiation of peroxidation (by rapidly clearing CO) and stimulate the upregulation of endogenous antioxidant defences.
Safety, Contraindications, and Practical Considerations
HBOT is a well-established medical procedure with a strong safety record when delivered by trained teams. The most common side effects are related to pressure equalisation in air-filled body cavities — particularly middle ear barotrauma — and are generally mild and transient. The single absolute contraindication of clinical significance is untreated pneumothorax. Relative contraindications include severe COPD with CO₂ retention, claustrophobia, and certain medications (such as doxorubicin) that become toxic under hyperbaric conditions.
Logistical reality: Not all hospitals have hyperbaric facilities. In regions where chambers are available, transfer of a haemodynamically stable CO patient for HBOT — even when it adds 1–2 hours to treatment — remains appropriate for patients meeting indications, given the prevention of neurological disability that might otherwise persist permanently.
The Pregnancy Exception: A Special Obligation
Pregnant women represent a population in whom the indications for HBOT are extended. Foetal haemoglobin (HbF) has an even higher affinity for CO than adult haemoglobin, and the foetal circulation — already operating at lower oxygen tensions — has very limited reserve. The elimination half-life of COHb in the foetus lags behind maternal clearance significantly, meaning that even after a mother’s COHb has normalised, the foetus may continue to carry dangerous levels.
Guidelines from the UHMS and major obstetric bodies recommend considering HBOT in pregnant patients with any symptomatic CO exposure, with a COHb above 15–20%, or in cases of foetal distress, regardless of the apparent severity of the mother’s presentation.
Prevention Remains the Foundation
While HBOT represents the most powerful pharmacological intervention once poisoning has occurred, the extraordinary toxicity of CO makes prevention paramount. Working carbon monoxide detectors — tested monthly and with batteries replaced annually — save more lives than any clinical intervention. Common sources include gas furnaces and boilers, petrol-powered generators used indoors or in attached garages, wood-burning stoves with blocked flues, and vehicle exhaust in enclosed spaces.
Public health campaigns and building codes mandating CO detectors in all sleeping areas have produced measurable reductions in CO poisoning mortality in jurisdictions where they have been enforced — reductions that dwarf what any treatment advance can achieve at scale.
Conclusion
Carbon monoxide poisoning is a medical emergency that proceeds at the molecular level long before its symptoms become apparent and long after the patient is removed from the source. Hyperbaric oxygen therapy remains the most evidence-supported means of rapidly clearing CO from hemoglobin and mitochondrial enzymes, supplying dissolved oxygen to endangered tissues, and interrupting the secondary neuroinflammatory cascades that cause the most disabling long-term consequences. For patients who meet established clinical criteria, timely access to an HBOT chamber is not a luxury — it may be the difference between full recovery and permanent neurological disability.
Key references: Weaver LK et al., N Engl J Med 2002; Thom SR, J Appl Physiol 2006; Hampson NB & Mathieu-Nolf M, Ann Emerg Med reviews; Undersea and Hyperbaric Medical Society Indications for Hyperbaric Oxygen Therapy, 2019 edition.


Leave a Reply
Your email is safe with us.